




Pressure injuries have a profound effect on sufferers and those around them – including caregivers and whānau. Caring for people with pressure injuries presents a significant challenge, understanding the background to these injuries can shed light on our current understanding today. This article aims to look at a brief history of the understanding and evolution of pressure injuries as we know them today.
Looking at the history of pressure injuries, the oldest term was “decubitus”, originally described as gangraena per decubitum in 1777 which meant “dead tissue due to lying down” (PPPIA, 2019). The term bedsore was documented by Florence Nightingale in 1859¹. This became more widely used after the publication of a book called Bedsore Biomechanics – which in turn led to the first conference on pressure injuries in 1975¹. In Europe the term pressure ulcer is w idely used, however, in New Zealand, Australia, South-East Asia, and America the term pressure injury is used¹.
idely used, however, in New Zealand, Australia, South-East Asia, and America the term pressure injury is used¹.
However, what is a pressure injury? According to the EPUAP (European Pressure Ulcer Advisory Panel) the definition of a pressure injury is; “a localized injury to the skin and/or underlying tissue, usually over a bony prominence, resulting from sustained pressure (including pressure associated with shear)” ¹.
When there is bony prominence the pressure on the skin can causes ischemia – the primary aggravator. Ischemia is when there is a restriction of blood flow to certain parts of the body, the pressure of the external force (in this case a bed or surface) on the bony part of the body causes this. The restricted blood flow results in a shortage of oxygen that is vital to cellular metabolism. Cellular metabolism is what is needed to help keep the skin tissue alive¹.
Another factor that causes a pressure injury is when there is skin cell deformation¹. The tissue is damaged only when the threshold for deformation is exceeded. This causes the cytoskeleton to break down, which is the structure that keeps the cells together. Cell death can occur rapidly and the breakdown of these cells can occur within minutes. This is opposed to Ischemia deprivation which occurs a lot slower.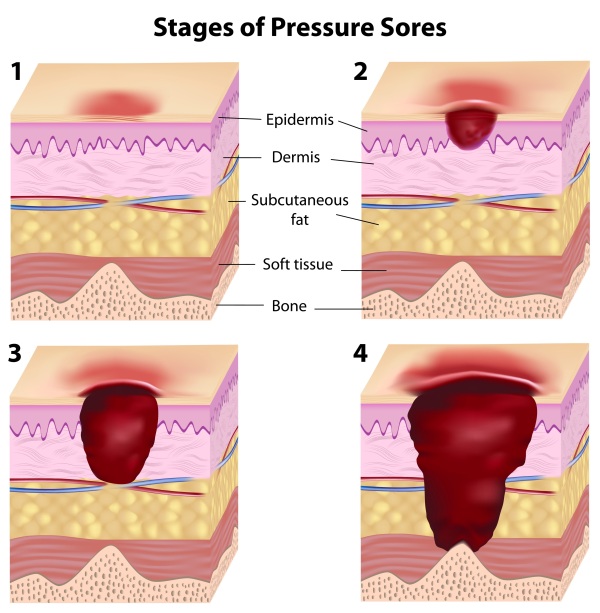
Once a pressure injury has been developed it is categorized in four different stages². The first is Category one, the intact skin with non-blanchable redness of a localized area usually over a bony prominence. Other signs of the area such as discolouration, oedema, warmer or cooler as compared to adjacent tissue may also indicate pressure injury. (Category 1 may be difficult to detect in individuals with dark skin tones. May indicate “at risk“ persons). Category 2 is Damage to the epidermis and/or dermis. The injury is superficial and may be visible as a blister on or an abrasion of the skin. Category 3 Involves damage to the full thickness of the skin and includes injury to, or necrosis of, the subcutaneous tissue layer, and may extend down to but not through the underlying fascia. Category 4 is Deep tissue damage, necrosis or damage to the muscle, bone or connective tissue with wound cavitations.
Pressure Injury prevention can be done by using specific relieving pressure care products such as air alternating mattresses, special cushions, turning schedules, good nutrition and staying hydrated². Active Healthcare is holding a Webinar titled Preventing and Treating Pressure Injuries: Best Practice Surface Selection. Join us on 29 March to learn about three of our leading mattress solutions.
¹ EPUAP/NPIAP/PPPIA, 2019, Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. https://www.internationalguideline.com/guideline
² Care of Sweden, 2022, Pressure Ulcers. https://www.careofsweden.com/pressure-ulcers/







